 Many patients suffering from COVID 19 are hypoxemic but not in distress and breathing comfortably in room air.This stage is called happy hypoxia.Hpoxemia is detected only after high index of suspician leads to SpO2 monitoring.
Many patients suffering from COVID 19 are hypoxemic but not in distress and breathing comfortably in room air.This stage is called happy hypoxia.Hpoxemia is detected only after high index of suspician leads to SpO2 monitoring.
Whenever there is less ventilation into the lung,there occurs a vasoconstriction in the pulmonary vessels as a compensatory response in poorly ventilated area of the lung..This is called hypoxemic Pulmonary vasocontrictor response(HPV).It has been seen that in COVID19 ,this HPV response is diminished with formation of intrapulmonary shunt(right to left) as demontrated by dual energy CT scan. This vasoplegic response is triggered by vasodilator prostaglandin,bradykinin and cytokines.
SARS Cov 2 virus,responsible for COVID 19, damages the endothelium of lung which express angiotensin converting enzyme II receptors, leading to formation of microthrombi in lung capillaries.There is extensive thrombi formation in arteries and capillaries leading to blockage of capillaries and arteries causing ventilation/perfusion mismatch and hypoxemia.This stage is called AVDS(acute vascular distress syndrome)
SARS Cov2 virus damages type 2 pneumocytes and in effect, basement membrane is denued which becomes covered by hyaline membrane consisting of fibrin and dead cells which impaires gas exchange.As the diffusion barrier becomes more pronounced,blood flow through pulmonary vessels increase during exertion.So there is less time for gas exchange during exertion causing hypoxemia.
In normal situations whenever there is less oxygen in the blood,it is sensed by carotid bodies which is situated at the bifurcation of commonl carotid artery..It gives signal to the respiratory centre situated in medulla oblongata which in turn sends signal to diaphragm via phrenic nerve to increase ventilation which is perceived as duspnea by patients.When the PaO2 is between 90 mmHg to 60 mmHg,there is no such response but as soon as the PaO2 drops below 60 mmHg ,immediately there is a signal exponentially, to increase the ventilation.But for this ventilatory response to occur, when the level of PaO2 is between 40mmHg to 60 mmHg,PaCo2 level must increase to above 39 mmHg to stimulate the carotid bodies.
SARS COV2 VIRUS BLOCKS the sensitivity of angiotensin converting enzyme 2 receptor present in carotid body .Therefore it can not sense hypoxia or hypercarbia unless it becomes critical.So,there is no signal to increase the ventilation and patients remain comfortable till the hypoxia becomes critical.This stage is called happy hypoxia.
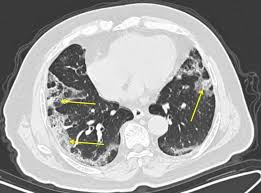
In the early stage of the disease,lung parenchyma is minimally involved which is evident by ground glass opacity in the peripheral regions of lung.In this stage ,vital capacity is maintained ,there is high compliance and low elastance of lung called L-Phenotype.At this stage there is low ventilatory response as the hypoxia is vascular in origin due to impairement of HPV and there is no dyspnea.
As the disease progresses,there is extensive involvement of lung parenchyma with increased ventilatory response,increased permeability of pulmonary capillaries with accumulation of fluid in interstitium(interstitial edema)and inspiratory pressure becomes more negative.This stage is called H-Phenotype with high elastance and low compliance.The transition from L-phenotype to H-Phenotype is precipitaed by more negative inspiratory pressure created by forceful inspiratory effort by patient during spontaneous breathing,called patient self inflected lung injury(P-SILI)
In case of fever, the oxygen dissociation curve is shifted towards right side, causing low SaO2 for a given PaO2, making the sensing of SpO2 by pulse oxymetry inaccurate as ,at low PaO2 level, SpO2 can underread by about 7 % if SaO2 is below 80%
In case of Diabetes and age more than 65 years the sensitivity of carotid body becomes less causing less ventilatory response.
IN NUTSHELL, at the initial stage of disease,there is minimal involvement of lung parenchyma,primarily the disease affects pulmonary vessels with less HPV response,AVDS,with development of rifht to left intrapulmonary shunt causing hypoxia,the virus decreases the sensitivity of carotid body to sense hypoxia and increase ventilatory response,shifting of oxygen dissociation curve to right causing low SaO2 for a given PaO2 due to high fever, all leading to less ventilatory response and patients remains comfortable till the critical stage.
REFERENCES:
1. Guan W, Ni Z, Hu Y, et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N Engl J Med. 2020;382(18):1708-1720. doi:10.1056/NEJMoa2002032
2. Mahjoub Y, Rodenstein DO, Jounieaux V. Severe Covid-19 disease: rather AVDS than ARDS? Crit Care. 2020;24(1):327. doi:10.1186/s13054-020-02972-w
3. Lang M, Som A, Mendoza DP, et al. Hypoxaemia related to COVID-19: vascular and perfusion abnormalities on dual-energy CT. Lancet Infect Dis. Published online April 30, 2020. doi:10.1016/S1473-3099(20)30367-4
4. Dhont S, Derom E, Van Braeckel E, Depuydt P, Lambrecht BN. The pathophysiology of ‘happy’ hypoxemia in COVID-19. Respir Res. 2020;21(1):198. doi:10.1186/s12931-020-01462-5
5. Ackermann M, Verleden SE, Kuehnel M, et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in Covid-19. N Engl J Med. 2020;383(2):120-128. doi:10.1056/NEJMoa2015432
6. Mahjoub Y, Rodenstein DO, Jounieaux V. Severe Covid-19 disease: rather AVDS than ARDS? Crit Care. 2020;24(1):327. doi:10.1186/s13054-020-02972-w
7. Mason RJ. Pathogenesis of COVID-19 from a cell biology perspective. Eur Respir J. 2020;55(4). doi:10.1183/13993003.00607-2020
8. Mo X, Jian W, Su Z, et al. Abnormal pulmonary function in COVID-19 patients at time of hospital discharge. Eur Respir J. 2020;55(6):2001217. doi:10.1183/13993003.01217-2020
9. Hopkins SR. Exercise Induced Arterial Hypoxemia: The role of Ventilation-Perfusion Inequality and Pulmonary Diffusion Limitation. In: Roach RC, Wagner PD, Hackett PH, eds. Hypoxia and Exercise. Advances in Experimental Medicine and Biology. Springer US; 2007:17-30. doi:10.1007/978-0-387-34817-9_3
10. Masi P, Bagate F, d’Humières T, et al. Is hypoxemia explained by intracardiac or intrapulmonary shunt in COVID-19-related acute respiratory distress syndrome? Ann Intensive Care. 2020;10(1):108. doi:10.1186/s13613-020-00726-z
11. Reynolds AS, Lee AG, Renz J, et al. Pulmonary Vascular Dilatation Detected by Automated Transcranial Doppler in COVID-19 Pneumonia. Am J Respir Crit Care Med. Published online August 6, 2020:rccm.202006-2219LE. doi:10.1164/rccm.202006-2219LE
12. Mohan R, Duffin J. The effect of hypoxia on the ventilatory response to carbon dioxide in man. Respir Physiol. 1997;108(2):101-115. doi:10.1016/S0034-5687(97)00024-8
13. Gattinoni L, Chiumello D, Caironi P, et al. COVID-19 pneumonia: different respiratory treatments for different phenotypes? Intensive Care Med. 2020;46(6):1099-1102. doi:10.1007/s00134-020-06033-2
14. Weisbrod CJ, Eastwood PR, O’Driscoll G, Green DJ. Abnormal ventilatory responses to hypoxia in Type 2 diabetes. Diabet Med J Br Diabet Assoc. 2005;22(5):563-568. doi:10.1111/j.1464-5491.2005.01458.x
15. Kronenberg RS, Drage CW. Attenuation of the ventilatory and heart rate responses to hypoxia and hypercapnia with aging in normal men. J Clin Invest. 1973;52(8):1812-1819. doi:10.1172/JCI107363
16. Tobin MJ, Laghi F, Jubran A. Why COVID-19 Silent Hypoxemia Is Baffling to Physicians. Am J Respir Crit Care Med. 2020;202(3):356-360. doi:10.1164/rccm.202006-2157CP
17. Kelman GR. Digital computer subroutine for the conversion of oxygen tension into saturation. J Appl Physiol. 1966;21(4):1375-1376. doi:10.1152/jappl.1966.21.4.1375
 It is very common question and very common mistakes by parents,regarding when and how a solid food is introduced to baby.All babies should exclusively be breast fed right from birth ,preferably starting within 30-60 minutes of birth till the age of 6 months.Some mother says that since the child is born through caesarean section(OPERATION),I have started the baby to feed through bottle with formula milk.This is not the correct reason to start formula feeds.Milk production is very less during initial 3 days of child birth but it is sufficient for the baby and it is highly nutrItious and immunobooster to the child.Milk production begins only when the baby starts sucking.If the baby sucks more ,the milk production will be more,if the child sucks less,the milk production will be less and if the child does not suck,there will be no milk production.
It is very common question and very common mistakes by parents,regarding when and how a solid food is introduced to baby.All babies should exclusively be breast fed right from birth ,preferably starting within 30-60 minutes of birth till the age of 6 months.Some mother says that since the child is born through caesarean section(OPERATION),I have started the baby to feed through bottle with formula milk.This is not the correct reason to start formula feeds.Milk production is very less during initial 3 days of child birth but it is sufficient for the baby and it is highly nutrItious and immunobooster to the child.Milk production begins only when the baby starts sucking.If the baby sucks more ,the milk production will be more,if the child sucks less,the milk production will be less and if the child does not suck,there will be no milk production.
 There is no specific treatment available for COVID 19,all over the world.
There is no specific treatment available for COVID 19,all over the world.
 REFERENCES;Pediatrc Pulmonology,online publication,June 2020
REFERENCES;Pediatrc Pulmonology,online publication,June 2020